Mini SUPERankle
What is the mini SUPERankle procedure?
The mini SUPERankle procedure is a term used to describe a supramalleolar osteotomy of the tibia and fibula in the face of a less severe deformity of the foot and ankle secondary to fibular hemimelia. Patients with a milder form of fibular hemimelia demonstrate adequate range of motion of the ankle but significant valgus deformity (foot kicking outwards on standing).
In more severe forms of fibular hemimelia, the foot and ankle present with a limited range of motion and are directed in a toe down (equinus) and outward twist or angulation (valgus). The ligaments, tendons and residual fibula (usually not seen on X-ray) are very tight and contracted. This type of deformity requires a comprehensive reconstruction of the foot and ankle that is called a SUPERankle procedure.
 Riley had a successful mini SUPERankle surgery combined with a SUPERhip procedure. Read about her treatment journey here.
Riley had a successful mini SUPERankle surgery combined with a SUPERhip procedure. Read about her treatment journey here.Less severe forms of fibular hemimelia can be treated with the mini SUPERankle surgical technique that has minimal to no soft tissue releases and simply redirects the distal tibial joint orientation. This is accomplished through a single incision over the lateral or outer aspect of the ankle and measures 5 cm (2 inch).
The mini SUPERankle surgery can be an isolated procedure for the patients with mild fibular hemimelia or combined with a more complex congenital femoral deficiency procedure such as a SUPERhip or rotationplasty. It is common to have a foot and ankle deformity that can be overlooked in the face of a more severe femoral or hip deformity. However, the foot and ankle deformity should be addressed simultaneously to maximize the success of the lower limb reconstruction.
What happens during mini SUPERankle surgery?
The following illustrations demonstrate the step-by-step technique for the mini SUPERankle procedure.
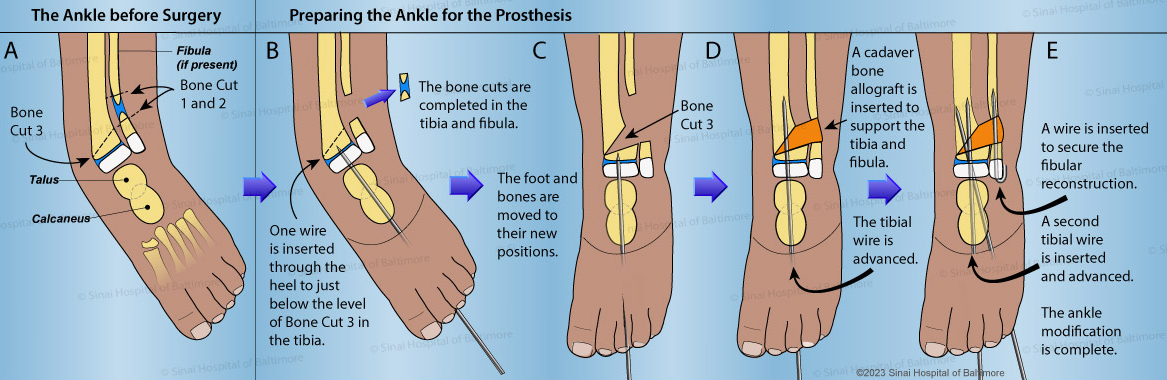
- A. The valgus (outward) orientation of the ankle is confirmed under X-ray. The dotted lines mark the planned bone cuts (osteotomies).
- B. Through the lateral incision, a small piece of the fibula is removed, creating a gap (Bone Cut 1 and 2). If this piece of the fibula is fibrous, the tissue is discarded. However, if the fibula is bone, the small fragment is preserved to serve as bone graft. The foot is placed in the maximally deformed position and then pinned to the level of the distal tibial bone cut. This makes the foot and distal tibial one stable “unit” for the correction. For a mild fibular hemimelia or a concurrent procedure with a hip reconstruction, the ankle is positioned in a neutral or foot flat position when viewing the foot/ankle from the side. If a rotationplasty is being performed, the ankle will function as a knee joint in the prosthesis. Therefore, the ankle is pinned in a toe-down position to simulate knee extension.
- C. Using the same lateral incision and working through the fibular gap, the distal tibial bone cut is performed (Bone Cut 3). It is directed obliquely to the growth plate to avoid causing a large bony prominence after the correction is completed. Once the tibial bone cut is completed, the foot and ankle are gently manipulated into the correct “normal” position.
- D. A cadaver bone allograft is inserted into the void created by the opening wedge osteotomy. The tibial wire is advanced, passing across the osteotomy site and stabilizing the new foot and ankle position.
- E. Additional wires are inserted to complete the stabilization of the osteotomy.
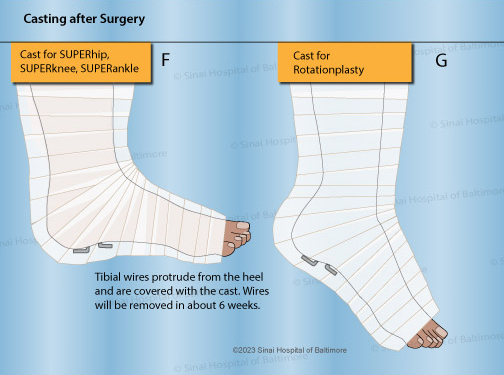
- F. The foot and ankle wires are bent and cut short outside of the skin. The foot is casted in a neutral position. The cast and wires remain in place for 6-8 weeks. Typically, the cast and wires are removed during a brief anesthesia/sedation.
- G. Alternatively, for SUPERankle procedures that are performed with concurrent rotationplasty of the lower limb, after the foot and ankle wires are bent and cut short outside of the skin, the foot is casted in a toe-down or plantar flexed position. This position simulates knee extension since the ankle joint becomes the new “knee joint.” The cast and wires remain in place for 6-8 weeks. The cast and wires are removed during a brief anesthesia/sedation.
Why choose the International Center for Limb Lengthening for mini SUPERankle surgery?
Our pediatric orthopedic team has extensive experience in performing this surgery. Your doctor will take the time to make sure you understand all your options and then will customize a treatment plan to meet your child’s specific needs.
Our patients benefit from our team-centered approach with world-renowned pediatric orthopedic surgeons, anesthesiologists with extensive experience working with pediatric patients, and specialized physician assistants, nurses and physical therapists. We also have a group of patient families who have children who have had SUPERankle and mini SUPERankle surgery that offer support through our International Center for Limb Lengthening (ICLL) Facebook Group, ICLL Families. We help patients achieve their best possible mini SUPERankle surgery result.