SUPERankle
What is a SUPERankle procedure, and when is it necessary?
The SUPERankle procedure is a comprehensive reconstruction of the foot and ankle. In severe forms of fibular hemimelia, the foot and ankle present with a limited range of motion and are directed in a toe down (equinus) and outward twist or angulation (valgus). The ligaments, tendons and residual fibula (usually not seen on X-ray) are very tight and contracted. The SUPERankle procedure is designed to correct this type of deformity.
The nickname “SUPER” was applied to several reconstructions for congenital limb deficiency. Each reconstruction consists of multiple procedures or steps to achieve the comprehensive joint reconstruction. These multiple steps were grouped together under the nickname “SUPER.” Patients with a milder form of fibular hemimelia who demonstrate adequate range of motion of the ankle, but significant valgus deformity (foot kicking outwards on standing) may be able to be treated with a mini SUPERankle procedure.
What is the ultimate goal of the SUPERankle procedure?
The ultimate goal of the SUPERankle procedure is to achieve a stable foot and ankle that can be placed flat on the ground with maintained range of motion in dorsiflexion and plantar flexion. (Dorsiflexion is when the front of the foot is flexed up and back towards the leg, while plantar flexion is a foot movement in which the foot flexes down towards the sole of the foot.)
What happens during SUPERankle surgery?
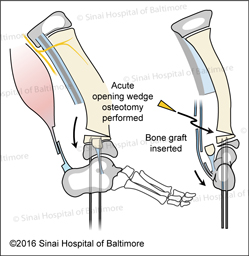
The SUPERankle procedure is a comprehensive release of the contracted soft tissues around the ankle joint with osteotomies (bone cuts) of the midshaft tibia (shin bone), distal tibia (right above ankle) and possibly the calcaneus (heel bone). This procedure aligns the foot and ankle and corrects the patient’s downward and outward foot deformity (equinovalgus deformity).
During the comprehensive release, the fibrous fibular anlage (the early remnant of the fibula that did not finish forming bone—can be fibrous, cartilage, or bone) is removed and used to reinforce the lengthened heel cord (Achilles tendon). At the same time, a tibial midshaft osteotomy is performed to straighten the lower leg bow. The skin dimple marks the apex or bend of the tibial deformity. This tibial bone cut can be used to straighten and lengthen the tibia 1-2 centimeters (0.4- 0.8 inches).
Since the ankle is mobile, the SUPERankle alignment procedure is performed first, usually between the ages of one and two years, and if lengthening is needed, the first lengthening would take place around the age of 3. During this first lengthening procedure, the tibia can gain up to 5 centimeters (2 inches) of length. If a SUPERankle and major lengthening were to be performed simultaneously, the ankle joint would stiffen.


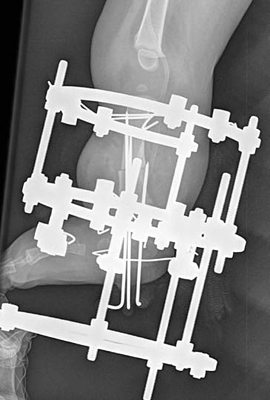
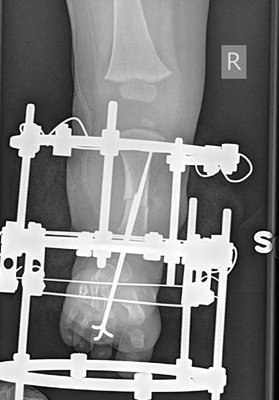


The SUPERankle alignment procedure can be performed with a simple Ilizarov external fixator that is applied to support the leg. This type of external frame does not require adjustments. The patient is able to weight bear/walk in this frame. However, the typical SUPERankle treatment uses a hinged Ilizarov fixation device that requires adjustments to straighten the tibial bone and lengthen 1-2 centimeters (0.4- 0.8 inches). It also allows full weight bearing.



What if the foot and ankle deformity returns?
One must understand that the initial reconstruction is a very complex set of procedures that is unique for each child. Sometimes a smaller revision surgery is required after the SUPERankle procedure. After the initial correction of the foot and ankle with the SUPERankle procedure, the foot can shift back to the outside. This gives the appearance that the child is walking on the inside ankle bone. This phenomenon can occur soon after the SUPERankle procedure when the child returns to weight bearing or can gradually appear as the child continues to grow. This recurrent type of deformity is unusual.
If the foot and ankle deformity returns soon after the initial procedure, it means that an underlying bony deformity was either under corrected or unmasked by the initial reconstruction. This unmasked deformity or recurrence can be addressed with a smaller revision surgery that requires a bone cut in the distal tibia or between the ankle and heel bone. Usually, the leg is placed in a cast for four to six weeks for healing and then the child is allowed to wear regular shoes.
The foot and ankle deformity that gradually reappears during early adolescence is addressed at the final surgical intervention, which usually occurs between 12 and 16 years of age. At the final surgical reconstruction, the leg lengths are equalized with a lengthening from the upper tibia and the foot/ankle position is corrected from the lower tibia. After this reconstruction is complete, the correction is permanent since the patient is nearing the end of growth.
Why choose the International Center for Limb Lengthening for SUPERankle surgery?
Our pediatric orthopedic team has extensive experience in performing this complex reconstructive surgery. Your doctor will take the time to make sure you understand all your options and then will customize a treatment plan to meet your child’s specific needs.
Our patients benefit from our team-centered approach with world-renowned pediatric orthopedic surgeons, anesthesiologists with extensive experience working with pediatric patients, and specialized physician assistants, nurses and physical therapists. We also have a group of patient families who have children who have had SUPERankle surgery that offer support through our International Center for Limb Lengthening (ICLL) Facebook Group, ICLL Families. We help patients achieve their best possible SUPERankle surgery result.