Club Hand
What is club hand?
Congenital longitudinal radial deficiency, otherwise known as radial club hand or radial dysplasia, is uncommon and affects less than 1 in 30,000 live births. The condition is relatively easy to diagnose as those with radial club hand have a physical deformity of the hand and/or forearm due to an absence or insufficient development of the radius bone, (one of the largest bones in the forearm extending from the elbow to the wrist). In addition, one or more fingers/thumb may be either missing or partially developed. Approximately one out of every two radial club hand patients has the condition in both limbs; this is called bilateral club hand.
There are no currently known causes for or factors contributing to this congenital (present at birth) deficiency. There are multiple syndromes that are associated with radial dysplasia. Syndromes related to radial dysplasia include: Thrombocytopenia-Absent Radius Syndrome (TAR), Fanconi anemia, Holt-Oram syndrome, Okihiro syndrome, Lacrimo-Auriculo-Dento-Digital Syndrome (LADD), Nager syndrome, Baller-Gerold syndrome, Richieri-Costa-Pereira syndrome, Roberts syndrome, and VACTERL association. Therefore, a thorough work up, consisting of a physical exam, ultrasounds of heart and kidneys, blood work and genetic testing, is necessary for all newborns with this condition.
 Our patient Anicka is pictured here before, during and after ulnarization treatment. For more about her patient experience, please see her story on our Patient Stories page.
Our patient Anicka is pictured here before, during and after ulnarization treatment. For more about her patient experience, please see her story on our Patient Stories page.What are the different types of club hand?
Radial club hand is classified into four types based on the severity of the defects and degree of radius bone present. Type 1 is the mildest form with type 4 being the most severe and common. The malformation or absence of bone in the lower arm, hand or wrist has a direct impact on the development of surrounding blood vessels, muscles and nerves so this classification system is designed to rate the impact of the complete condition.
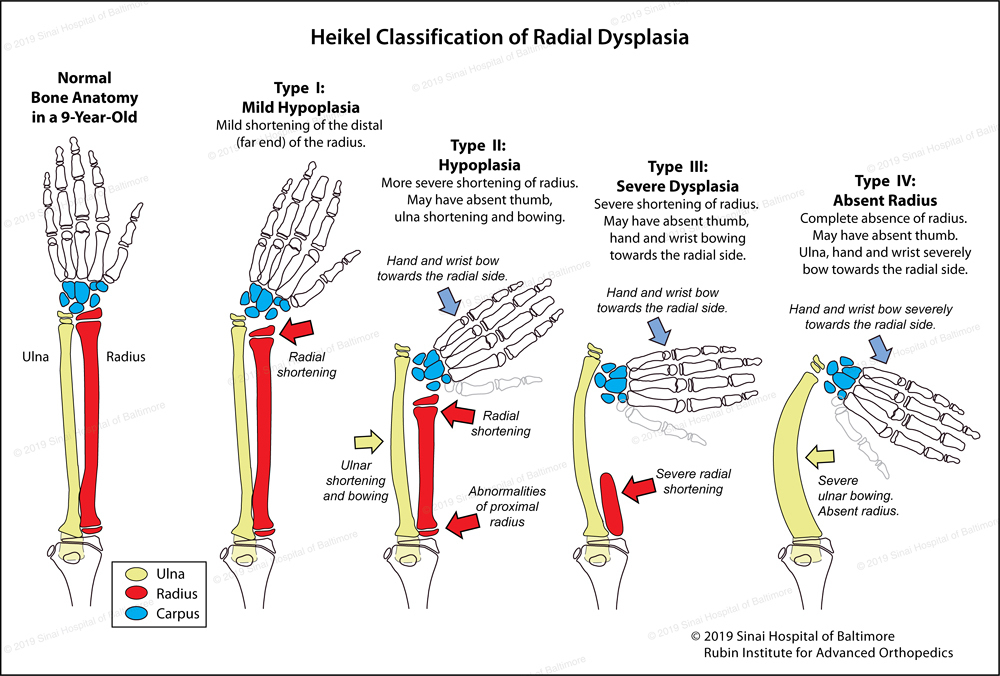
According to the Heikel classification system of the severity of radial club hand:
- Type 1: Mild shortening of the distal radius
- Type 2: More severe radial shortening—ulna (forearm bone parallel to the radius) shortening and bowing may also be present
- Type 3: Severe radial shortening and radial deviation of the hand and wrist
- Type 4: Complete absence of the radius with severe radial deviation of the hand and wrist.
The Heikel classification is similar to the Bayne and Klug classification system; the differences are not clinically significant.
What happens when radial club hand is not treated?
Children who are not treated for radial club hand may experience decreased functionality due to the persistent deformity. It should be noted that if neglected, corrective treatment is significantly more challenging in adults.

How is radial club hand treated?
At the Rubin Institute for Advanced Orthopedics, our expert pediatric orthopedists will provide the family with a comprehensive treatment plan which may include an initial surgery—ulnarization—to correct the deformity and achieve normal alignment of the wrist. The least severe type of radial club hand, type 1, is typically initially treated non-surgically with the use of splints, casts and occupational therapy. Eventually these patients may require surgical intervention later in childhood or at the end of skeletal growth (age 14-16 years). Surgical intervention is typically performed much earlier in patients with higher classification types of radial club hand; the goals are to create a stabilized and mobile wrist, a functioning hand, the reconstruction or creation of a thumb (pollicization), and to ensure adequate long-term bone growth. This highly specialized and complex surgery is typically performed in stages during the first few years of a child’s life.
What are the various surgical treatments for the different types of club hand?
The International Center for Limb Lengthening’s recommends different courses of treatment for the different severity classes:
Type 1 Radial Dysplasia
This type of radial dysplasia is treated by lengthening the radius through an osteotomy (bone cut) in the distal (lower wrist end) part of the radius. This strategy grows the radius to support the wrist bones (carpus) and correct the relationship between the radius and ulna. This is accomplished by either a one or two stage treatment plan in the mid-childhood ages. The first stage is performed by application of an external fixation device to the hand and wrist to gradually reposition them into a normal position if needed. The second stage consists of adjusting the external fixation to hold the wrist and hand in the corrected position and beginning to lengthen the radius through a distal radial osteotomy. This type of strategy usually needs to be repeated towards the end of growth to accomplish permanent correction. The end of long bone growth usually occurs around the age of 14 for females and age 16 for males.
Type 2 Radial Dysplasia
This type of radial dysplasia falls in between the above treatment strategy and the procedure called ulnarization (described under types 3 and 4 below). The vast majority of the type 2 radial dysplasia patients seen at the International Center for Limb Lengthening have significantly abnormal growth areas at both ends; (the proximal upper end and distal lower end of the radius. This causes significant growth arrest in the radius and overt shortening during growth. This limits the ability to lengthen the radius enough to make the type 1 surgical strategy viable and successful in these type 2 cases. Because radius lengthening is so challenging, and because the deformity often reoccurs very quickly with this method, the International Center for Limb Lengthening instead uses ulnarization to treat patients with type 2 radial dysplasia.
Type 3 and Type 4 Radial Dysplasia
The International Center for Limb Lengthening has treated both of these severe types of radial dysplasia successfully with ulnarization. This procedure is a modification by Dr. Dror Paley of Dr. Buck Gramko’s radialization procedure. There are multiple differences in both surgical strategy and surgical technique when comparing ulnarization to radialization. Essentially, the hand and wrist bones are moved towards the small finger side (ulnar side) of the ulna. The deforming forces that caused radial club hand are then converted into stabilizing forces using the distal ulna (lower end of the forearm bone) as a fulcrum (pivoting point). The International Center for Limb Lengthening has made several positive modifications to both the technique and treatment protocol. This surgery is usually performed between 12-18 months of age, (although it can be done on children as old as ages six-eight years), and it is followed by pollicization if needed. If a patient is over eight years old, the deformity can still be addressed with Ilizarov wrist reconstruction. For more details about ulnarization surgery, please see our ulnarization treatment page.
Although some institutions use other procedures such as radialization and centralization, our center has had better results using ulnarization. We have had no recurrence of the deformity since we started performing ulnarization surgery in 2003. This procedure also preserves future growth of the distal ulna by allowing the bone to grow for many years after surgery. The results are a hand in a more functional position, stability of the deformity, improved grip strength and a mobile wrist. These advantages are not typically possible with centralization or radialization procedures. In ulnarization surgery, an external fixation device is used post-operatively to maintain the corrected position for three months.
Videos


Why choose the International Center for Limb Lengthening for treatment of club hand?
Deformity correction is a complex process. Your doctor at the International Center for Limb Lengthening will take the time to make sure you understand all your options and then will customize your treatment to meet your child’s specific needs. Our ulnarization treatment provides many advantages over more commonly performed centralization and radialization procedures. Our patients also benefit from our team-centered approach with world-renowned pediatric orthopedic surgeons, anesthesiologists with extensive experience working with pediatric patients, and specialized physician assistants, nurses and physical therapists. We also have a large group of patient families who have children undergoing radial club hand treatment that offer support through our International Center for Limb Lengthening (ICLL) Facebook Group, ICLL Families. We help patients with radial club hand achieve their best possible result.
![]()
Chat with a doctor about club hand
Our doctors hold free monthly chats on various subjects, including club hand. Click here for more information about our monthly chats.