Dwarfism
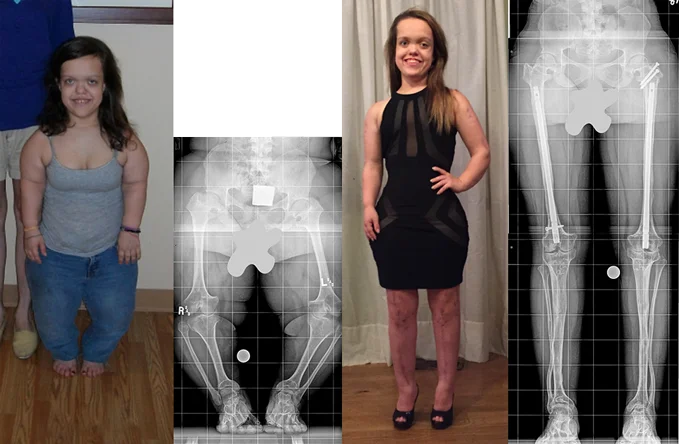 Chandler, a patient with achondroplasia, started her lengthening treatments at the International Center for Limb Lengthening at the age of 16. The first photo and X-ray show her before treatment, and the second photo and X-ray show her after one arm lengthening and two leg lengthening treatments. She started at her mature height of 3’10” and is now 4’11. She gained 13 inches of height and 4 inches of arm length.
Chandler, a patient with achondroplasia, started her lengthening treatments at the International Center for Limb Lengthening at the age of 16. The first photo and X-ray show her before treatment, and the second photo and X-ray show her after one arm lengthening and two leg lengthening treatments. She started at her mature height of 3’10” and is now 4’11. She gained 13 inches of height and 4 inches of arm length.What is dwarfism?
Bone dysplasia, also called skeletal dysplasia, is irregular growth of the bones from disorders or abnormal growth of the growth plates that causes short stature and disproportionate limb size—what we commonly call dwarfism. Over 200 conditions can cause dwarfism, but the most common is achondroplasia despite it being rare itself (occurring approximately once out of every 25,000 births. A dwarf or little person is an adult whose height is less than 4 feet 10 inches (147 cm). Most females with achondroplasia naturally grow to a height of 4 feet 2 inches (128 cm) and males grow to a height of 4 feet 4 inches (134 cm). An achondroplastic dwarf’s arms and legs are usually short compared with the head and trunk of the body. This shortness is predominantly in the upper arms and thighs. Many people with dwarfism also have lower extremity deformities including bowlegs and other knee or ankle problems that can make walking difficult and painful and can increase the likelihood of degenerative joint disease in the future. The humerus (upper arm) is shortened and curved at the elbow which prevents full extension of the elbow.
What are some of the daily living challenges?
Everyday items in our society are designed based on a minimum height of 5 feet (152 cm). Door knobs, light switches and car gas and brake pedals are out of reach for most people with dwarfism. Little people also have shorter arms, which can make personal hygiene difficult, especially as they age and back and spine mobility decreases. People with dwarfism who drive are vulnerable to airbag injuries due to the short distance they are from the steering wheel and airbag. Turning off the airbag, however, increases the risk of serious injury from the driver’s chest hitting the steering wheel column.
Not every patient with dwarfism requires treatment; it is a very personal decision made after weighing the risks and benefits. Many people with dwarfism use assistive devices to help them reach things and complete daily tasks (e.g., pedal extensions for driving, stools to reach high cabinets and counter tops). Some choose to just have their limb deformities corrected and to have their arms lengthened to be long enough for self-care.
Video: Limb Lengthening for Dwarfism
What are the goals of treatment?
As stated previously, not everyone with dwarfism requires treatment; it is a personal decision that must be made after weighing the risks and benefits. At the International Center for Limb Lengthening, we consult with each patient to determine his/her goals and needs. Our most common goals of treatment are:
- to obtain a functional height, normally between 4 feet and 10 inches (147 cm) and 5 feet and 2 inches (157 cm);
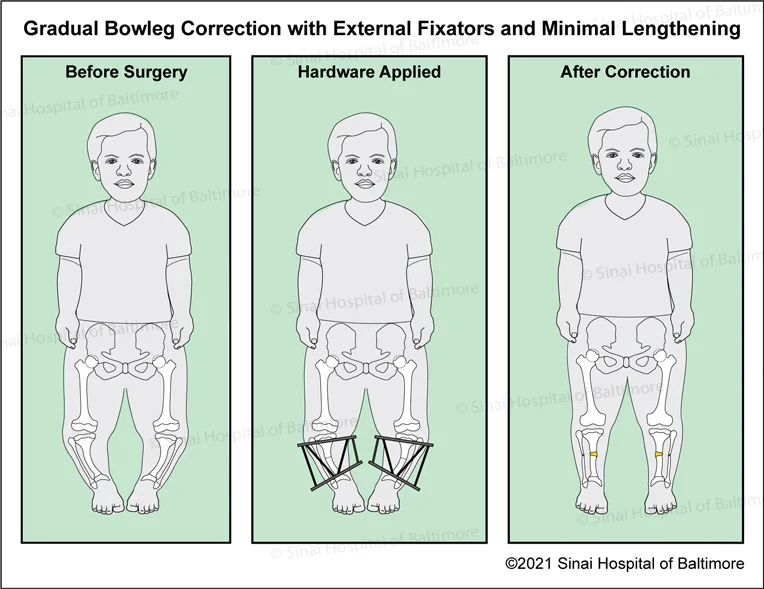
- to correct deformities like bowlegs to improve walking;
- to lengthen the arms to a functional length for self-care and driving; and
- to gain secondary psychological benefits from a more positive body image and body function.
For patients who elect to lengthen, after undergoing several phases of lengthening at the International Center for Limb Lengthening, most girls achieve a height of 5 feet (152 cm) and most boys achieve a height of 5 feet 2-4 inches (157-163 cm). However, our goal is not only to increase height and arm length, but also to correct deformities of the ankle, knee, hip, spine and elbow. For example, some people with dwarfism have an increased curve of the lower spine called hyperlordosis that results in “sway” back. This curvature in the spine can cause the spaces that the spinal cord and nerves pass through to become narrowed during adulthood resulting in spinal stenosis, which can cause pain or lack of sensation in the legs. We decrease the curvature of the spine by correcting hip deformities, which helps patients avoid problems later in life.
Lower extremity alignment in patients affected by achondroplasia varies from person to person. While some patients already have normal alignment and are not at risk for knee damage, other patients are affected by mechanical axis deviation, placing them at increased risk for wear and tear on the knee. Malalignment of the lower extremity is an independent risk factor for developing arthritis. Patients with achondroplasia are at increased risk for bowleg deformity, which can also lead to increased stress on the lateral (outer) aspect of the knee and discomfort during movement.
Our approach at the International Center for Limb Lengthening is to focus on individual patient goals while optimizing the long-term outcome. Patients who do not want to undergo lengthening benefit from isolated deformity correction. Patients who also wish to pursue lengthening will undergo deformity correction in the initial surgical procedure.
How do our doctors treat dwarfism?
The International Center for Limb Lengthening’s pediatric orthopedics physicians have partnered with the Pediatric Endocrinology Division at the Herman & Walter Samuelson Children’s Hospital at Sinai to offer BioMarin’s VOXZOGO, also known as vosoritide, an injectable prescription medication that has been FDA-approved to increase linear growth for children with achondroplasia who are five years of age and older and still have open growth plates. For more information about VOXZOGO treatment, please contact our doctors or Dr. Debra Counts or Dr. Albara Marwa of Sinai’s pediatric endocrinology division at 410-601-8331.
Limb deformity correction can occur at any age. Limb lengthening, with or without deformity correction, is not recommended for children at ages 4 or 5, because a certain maturity level is necessary for a child to have a successful lengthening treatment, and the treatment itself may interfere with natural bone growth at this stage. Severe deformities like bowing of the legs may be addressed in these early years, and some patients have spinal issues that need to be addressed prior to lengthening.
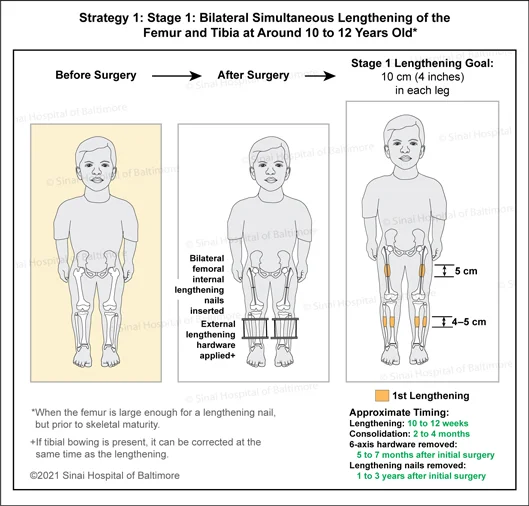
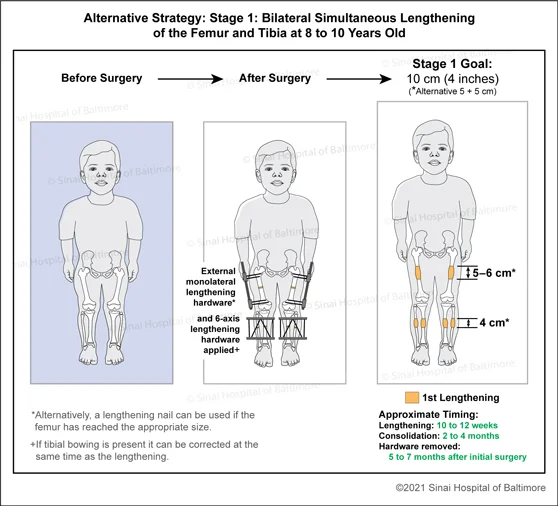
While some patients choose to start in their late teens or early twenties, it is much harder to achieve as much height starting that late in life. We recommend that patients ideally have their first lengthening (with or without deformity correction) surgery between ages 8 and 10, and they will ultimately undergo three stages of treatment over the course of their childhood and adolescence. The approximate total increase in lower limb length is 8-10 inches (20-25 cm) and the approximate total increase in upper limb length is 3-4 inches (7.6-10 cm). See our limb lengthening section to learn about this process.
First Stage: First Leg Lengthening at Ages 8-10 or 10-12
- Surgery:
- Examination under anesthesia.
- Release of the tight bands around the knee.
- Bone is cut (osteotomy) and internal Precice rod or external fixator is applied to both femur (thigh) bones to ultimately achieve 2.5 inches (6 cm) of growth, and an external lengthening device to both tibia (shin) bones to eventually achieve 1.5 inches (4 cm) of growth for a total of 4 inches (10 cm).
- Note: This surgery is usually done all at once, but the legs may be staged a week apart if it would benefit the patient to do so, (can be dependent on spinal cord monitoring, blood loss and other factors).
- Post-Surgery:
- Expect to spend 3-4 days in the hospital.
- Then spend 5-7 days of rest before lengthening begins.
- Then spend 10-12 weeks in the distraction (lengthening) phase gaining approximately a centimeter every 2 weeks while doing physical therapy 3-5 days a week for 1-2 hours a day. This intensive physical therapy must be done for the lengthening to succeed, and because it is so specialized, it must be done at the Rubin Institute.
- During this lengthening period, the patient will need to be seen at the International Center for Limb Lengthening clinic every 2 weeks. This type of extensive lengthening requires close clinical follow up to achieve the best results and avoid complications.
- During this distraction phase:
- Then for 2-4 months, the bone needs to consolidate and heal. This phase can be completed at home and X-rays can be sent intermittently.
- In the consolidation phase:
- When the bone is solid, the patient will return to the clinic.
- Removal:
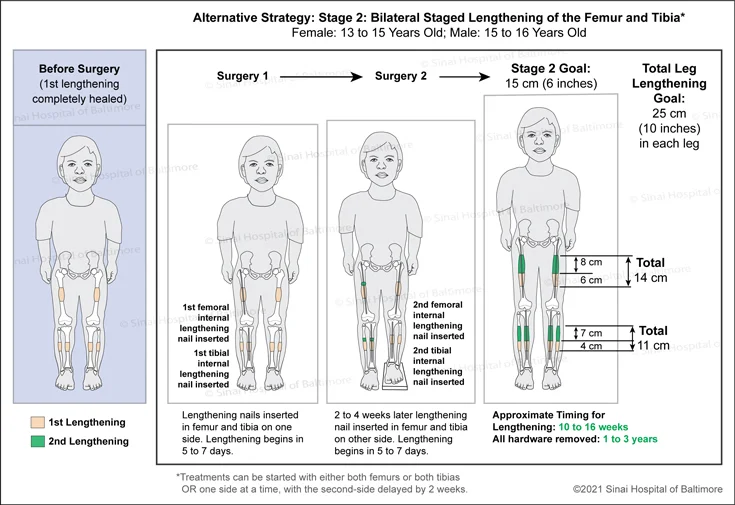
Second Stage: Second Leg Lengthening at Age 13-14 for Girls and 15-16 for Boys
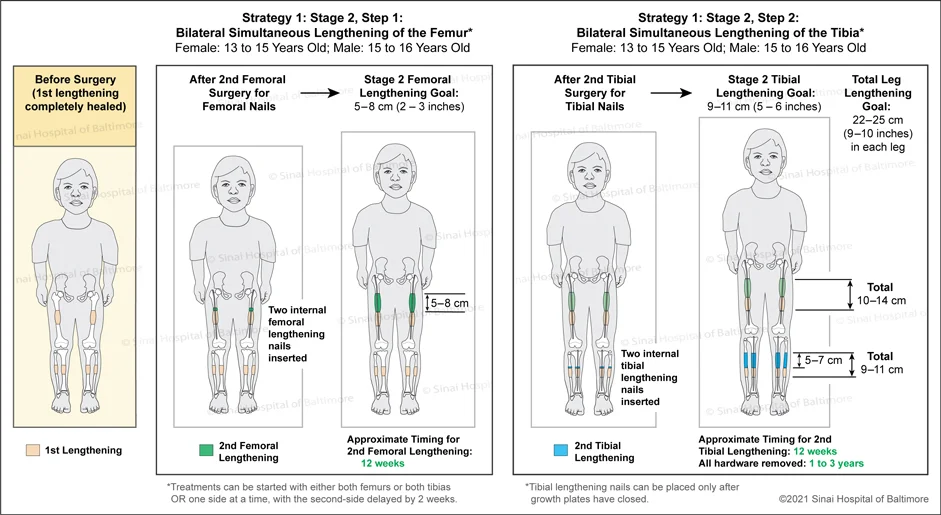
- Surgery:
- Insert Precice internal rods to lengthen both femur bones 3 inches (8 cm) and both tibia bones 2.8 inches (7 cm) for a total increase in leg length of 5-6 inches (12.7-15 cm).
- Preparatory series of soft tissue releases
- Note: This surgery is normally done in 2 stages, first the tibia bones and then the femur bones, 2-4 weeks apart.
- Note: Alternatively, treatment can be started on one side at a time, with the second side delayed by 2 weeks.
- Post-surgery:
- Same as first lengthening (see above).
Third Stage: Arm Lengthening* at Age 16-18
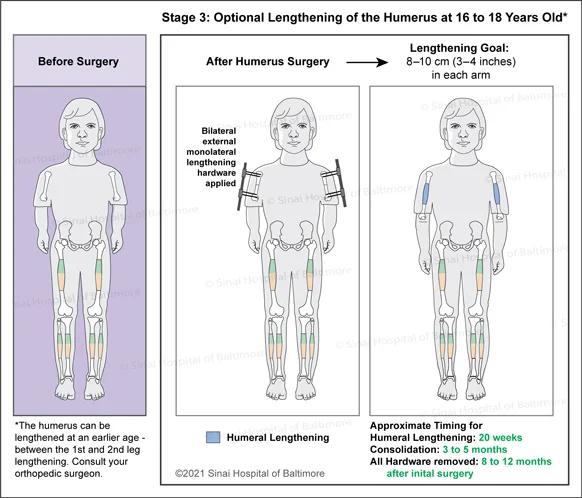
- Surgery:
- Apply external fixators to humerus bones to lengthen both arms 4 inches (10 cm).
- Perform radial nerve decompression
- Surgery takes 3-4 hours.
- *Note: The main goal of the arm lengthening is to achieve a functional length. Some patients may want to correct flexion deformity (inability to fully extend) due to elbow contractures but not lengthen. They opt for a different surgery where the bone is cut at a different level with the goal of correcting the elbow flexion deformity. This surgery enables the patient to achieve only 1.2 inches (3 cm) of length. Patients who do choose to lengthen the arms may also opt to have this procedure as a second arm surgery after their lengthening is completed.
- Post-Surgery:
- Stay 1-2 nights at the hospital, and then plan to stay at least 1-2 weeks in Baltimore.
- Lengthening starts on the 7th day after surgery. It typically takes 20 weeks to lengthen 10 cm. You must be seen in clinic every 2-4 weeks.
- After approximately 5 months of lengthening, you will spend 3-5 months healing for the bone to consolidate.
- During the active lengthening phase, you will do physical therapy 2-3 days a week to maintain shoulder, elbow and hand function. You must limit lifting to 1-3 pounds (.45-1.4 kg), and cannot lift anything with the arms fully extended, but can otherwise go to school and do activities.
- The external fixators are removed once the lengthening segment has fully consolidated and shows up as being fully healed on X-ray examination.
- Fifty percent of the time, rods are put in the bone at the time of removal to help stabilize bone growth. This is decided during surgery if the lengthening segment is “narrowed” or one to two sides of the bone are not fully healed.
Fourth Stage:
- The International Center for Limb Lengthening generally does not recommend a third round of leg lengthening if the patient has successfully met the goals of their first two leg lengthening treatments, but this can be an option for some patients.
Why choose the International Center for Limb Lengthening for treatment of issues associated with achondroplasia and other forms of dwarfism?
Limb lengthening and deformity correction are complex processes. Your doctor at the International Center for Limb Lengthening will take the time to make sure you understand all your options and then will customize your treatment to meet your specific needs. Our patients benefit from our team-centered approach with world-renowned pediatric and adult orthopedic surgeons as well as specialized physician assistants, nurses and physical therapists. Our anesthesiologists also have extensive experience in working with children and adults with dwarfism conditions. We help patients with achondroplasia and other forms of dwarfism achieve their best possible result.
![]()
Chat with a doctor about dwarfism
Our doctors hold free monthly chats on various subjects, including dwarfism. Click here for more information about our monthly chats.