Rotational Deformities: In-toeing and Out-toeing
What are rotational deformities of the foot and leg?
Rotational deformities occur when the foot or a leg bone are turned or twisted inward or outward, and this causes the feet to turn inward or outward rather than pointing straight ahead. In-toeing and out-toeing are some of the most common concerns seen in an orthopedic deformity practice. There is often no pain associated with the rotational difference, but this is not always the case.
How are rotational deformities diagnosed and treated?
Most commonly, rotational deformities are noticed by parents of young children and brought to the attention of pediatricians who refer the patient to an orthopedic specialist. The evaluation and treatment of rotational differences depend primarily on two factors: the patient’s age and associated symptoms. The orthopedic specialist will conduct a thorough physical examination to determine the cause of the rotational deformity and will get the family and patient history to determine risk factors for other orthopedic problems. Older patients with rotational deformities often present with hip or knee pain, and they only find out about the rotational difference in retrospect.
What is in-toeing?
In-toeing is when the feet turn inward instead of pointing straight ahead. In-toeing is most commonly linked to one of three factors: a bean-shaped foot (metatarsus adductus), an internal twist in the lower leg (internal tibial torsion), or an internal twist of the femur (femoral anteversion).
- Metatarsus adductus (when the foot turns inward): For the bean-shaped foot, examination focuses on the flexibility of the foot and screening for associated problems. Metatarsus adductus can be treated with special braces for the foot, which help form the foot into a more typical shape. This process is similar to, but less involved, than treatment of clubfoot. Regular follow-up appointments are scheduled to be sure that the brace is fitting well and that the foot is responding appropriately. In rare cases, a cast is placed.
Infants with this foot shape should be evaluated for hip dysplasia, as it is often considered a “packaging disorder.” In plain terms, this means that the space available for the baby in the womb was small enough that the baby was packed in tightly, limiting motion and resulting in the shaping of the foot. Checking for hip dysplasia is most important in firstborn female babies, especially if there is a family history of dysplasia. In older children and adults, metatarsus adductus is typically an issue of appearance. In some instances, surgical treatment is needed for patients with other symptoms.
- Metatarsus adductus (when the foot turns inward): For the bean-shaped foot, examination focuses on the flexibility of the foot and screening for associated problems. Metatarsus adductus can be treated with special braces for the foot, which help form the foot into a more typical shape. This process is similar to, but less involved, than treatment of clubfoot. Regular follow-up appointments are scheduled to be sure that the brace is fitting well and that the foot is responding appropriately. In rare cases, a cast is placed.
- Internal tibial torsion (when the shin bone turns inward): When the rotational difference is located in the lower leg, examination focuses on determining the level of the rotational difference, the magnitude of the difference, as well as screening for any associated differences. Patients may notice that when they stand and walk, the knee points forward, but the foot points in. The amount of torsion in the tibia (shin bone) is recorded by having the patient lie on their stomach and then the angle between the foot and the thigh is measured. Often, some degree of metatarsus adductus is present, which worsens the overall appearance.Treatment of metatarsus adductus in small children is generally not indicated, as braces have been shown to be ineffective. Often, the difference does not lead to symptoms, and can be observed. Severe deformity that limits the ability to walk with a normal foot progression angle can lead to discomfort as adjacent joints struggle to accommodate the difference.
Unfortunately, bracing for internal tibial torsion is ineffective. Treatment requires an osteotomy (bone cut) to realign the bone and fixation with a plate, rod, or external fixator. The fixation method depends on the patient’s age, associated differences, and other variables. Once the bone is healed, patients can return to unrestricted activity. Treatment is generally deferred until at least age 8, when an adult gait pattern is typically established, and compensatory mechanisms can be evaluated. In adults, physical therapy may be helpful for evaluating gait mechanics and other sources of pain, but surgical treatment is the only way to change the rotational alignment of the bone.
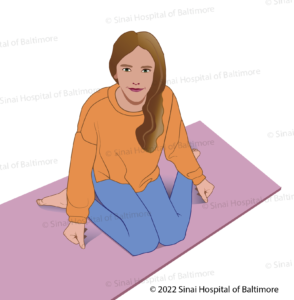
This girl is in the W-sitting position.
- Internal tibial torsion (when the shin bone turns inward): When the rotational difference is located in the lower leg, examination focuses on determining the level of the rotational difference, the magnitude of the difference, as well as screening for any associated differences. Patients may notice that when they stand and walk, the knee points forward, but the foot points in. The amount of torsion in the tibia (shin bone) is recorded by having the patient lie on their stomach and then the angle between the foot and the thigh is measured. Often, some degree of metatarsus adductus is present, which worsens the overall appearance.Treatment of metatarsus adductus in small children is generally not indicated, as braces have been shown to be ineffective. Often, the difference does not lead to symptoms, and can be observed. Severe deformity that limits the ability to walk with a normal foot progression angle can lead to discomfort as adjacent joints struggle to accommodate the difference.
- Femoral anteversion (when the thigh bone turns inward): When the rotation difference is in the thigh, the examination focuses on determining the level of the difference, the magnitude of the difference and screening for any other associated problems. Patients may notice that when they stand and walk, both the knee and the foot point inward. Excessive anteversion is often evident in patients who W-sit. Excessive anteversion is confirmed on physical examination by rotating the hips while the patient lies on their stomach. The angular range of motion is recorded carefully.
In young children, the treatment is just monitoring, as many children will improve their rotational alignment with age. Braces are ineffective. Surgical treatment is generally delayed until age 8 to allow time for the alignment to spontaneously correct itself. Also, by the age of 8, an adult gait pattern is typically established, and compensatory mechanisms can be evaluated. Treatment is generally completed by cutting the bone (osteotomy) and realigning it over a rod inside the bone. Patients are allowed to put full weight on the leg during recovery. Once healed, patients can return to full unrestricted activity. In adults, physical therapy may be helpful for evaluating gait mechanics and other sources of pain, but surgical treatment is the only way to change the rotational alignment of the bone.
What is out-toeing?
Out-toeing is when the feet point outward while walking. The most common causes are: flexible flat foot (loss of foot arch when standing), external tibial torsion (external twist at the shin bone), or femoral retroversion (external twist at the thigh bone).
- Flexible flatfoot: Flexible flatfoot is commonly noticed by parents in young children. The arch of the foot “collapses” when the child stands and is restored when the foot is not on the ground. The arch also returns when the child stands on tiptoes. Flexible flatfoot is usually not painful, and as long as good motion is maintained in the ankle (flexibility of the heel cord), symptoms are very uncommon. In some circumstances surgical procedures may be needed, including lengthening of the heel cord and osteotomies to correct the shape of the foot. In contrast to adult-acquired or rigid flatfoot, the long-term prognosis is for continued good function without surgical intervention.
- External tibial torsion (when the shin bone is twisted outward): External tibial torsion occurs when the external twist is located in the lower leg. Patients may notice that while their knee is pointed forward, the foot points out. External torsion is less common than internal torsion, but it is similar in that bracing is not effective for it either. The doctors’ physical examination also focuses on measuring the amount of rotation. The “thigh-foot angle” is recorded with the patient lying on their stomach and the knee bent to 90 degrees.
Surgical treatment is warranted when symptoms are present. Symptoms often occur if patients have difficulty getting their foot to a “forward” orientation, resulting in stress in the muscles of the hip which compensate for the abnormal foot progression angle. Knee pain is also possible. In adults, physical therapy and/or activity modification may be helpful in mitigating the symptoms, but surgical treatment remains the only option to change the underlying difference. Surgery entails cutting the bone, rotating the leg and fixing the bone with a plate, screws, internal rod or external fixator.
- External tibial torsion (when the shin bone is twisted outward): External tibial torsion occurs when the external twist is located in the lower leg. Patients may notice that while their knee is pointed forward, the foot points out. External torsion is less common than internal torsion, but it is similar in that bracing is not effective for it either. The doctors’ physical examination also focuses on measuring the amount of rotation. The “thigh-foot angle” is recorded with the patient lying on their stomach and the knee bent to 90 degrees.
- Femoral retroversion (when the thigh bone is twisted outward): Femoral retroversion occurs when the external rotation is in the thigh. Patients notice that their foot and kneecap both point externally when they walk. Physical examination for rotation of the femur is done with the patient lying on their stomach, and the knee bent to 90 degrees. The leg is then rotated to its maximum internal and internal positions, and this is recorded. Femoral retroversion is a common component of congenital femoral deficiency, but most patients with retroversion do not have femoral deficiency.
In young children, treatment is observation. By age 8, an adult-like gait has typically been established, and treatment becomes an option. Some patients will have pain in their hips or knees as the body tries to accommodate the rotational difference of the femur. Physical therapy and activity modification may be helpful. Surgical treatment in the form of osteotomy is the only way to change the underlying problem and is necessary when symptoms are not relieved by other methods. Treatment entails cutting the bone, rotating the leg, and fixing the leg with an internal rod.
A combination of femoral anteversion and external tibial torsion is present in what is known as “miserable malalignment.” This entity is also known as pan-genu torsion. Patients may notice that when their foot is forward, their knee points internally. Patients will have a similar running gait to patients with femoral anteversion. Knee pain is the typical symptom, although it is not always present. Physical therapy and/or activity modification may be helpful in alleviating symptoms. Surgical treatment is generally used for cases that do not improve with therapy. Depending on the degree of rotation in the femur and tibia, correction of one or both bones may be needed. Careful physical examination is necessary to ensure optimal realignment.
How are rotational deformities surgically corrected?
For rotational correction, surgeons at the International Center for Limb Lengthening use a technique developed at our institution known as fixator-assisted nailing or fixator-assisted plating. The use of a temporary stabilizing device in the operating room allows for very careful realignment and correction. The fixator-assisted technique can be used for many deformity correction surgeries, and it is especially important in rotational correction of the femur.
Why choose the International Center for Limb Lengthening for treating rotational deformities of the foot and leg?
The International Center for Limb Lengthening is world-renowned for its expertise in both foot and leg bone deformity correction. Your doctor will take the time to make sure you understand all your options and then will customize the treatment to meet your specific needs. Our patients benefit from our team-centered approach with world-renowned orthopedic surgeons and specialized physician assistants, nurses and physical therapists. We help patients with rotational deformities of the foot and leg achieve their best possible result.