Fibrous Dysplasia
What is fibrous dysplasia?
Fibrous dysplasia is a condition in which parts of normal bone are replaced by weaker bone or fibrous tissue that is susceptible to fracture and deformity. It is a type of benign (non-cancerous) bone tumor which most commonly presents in childhood or young adulthood. The presentation can vary from a patient without symptoms being diagnosed incidentally (i.e., unintentionally found during evaluation for another medical issue) to a patient who has multiple bones involved, causing pain, swelling, or fractures. Most commonly, a single bone is affected, which is typically discovered as an incidental finding.
The destruction of cells in the body, including bone, is called lysis. Hence, lytic lesions are the byproducts of bony destruction in fibrous dysplasia. In adulthood, there is a 1% chance of malignant (cancerous) transformation of these lytic lesions. The most commonly involved areas include the long bone in the thigh (femur), the shin bone (tibia), the ribs and the bones of the skull.
Orthopedic complications that can arise as a result of fibrous dysplasia include fractures, angular bone deformities, pseudarthrosis and limb length discrepancy. Fibrous dysplasia lesions can cause the bone to deform gradually, resulting in crooked or curved bones.
Fibrous dysplasia can also involve other organ systems, such as the skin and the hormone-producing endocrine system. Patients may have areas of darkly pigmented skin called café-au-lait spots. Endocrine conditions may include elevated levels of growth hormone, abnormal levels of the thyroid hormone and early (precocious) puberty in girls. McCune-Albright syndrome is associated with fibrous dysplasia; the condition involves multiple symptoms including fibrous dysplasia and often café-au-lait skin spots and endocrine system problems.
What causes fibrous dysplasia and how common is it?
Fibrous dysplasia is very rare and is caused by a genetic mutation; however, there is no evidence to suggest that it is hereditary.
How is fibrous dysplasia diagnosed?
The diagnosis of fibrous dysplasia involves both clinical and X-ray findings. A thorough history and physical is typically the first step. X-rays are also used to aid in the diagnosis, with typical findings showing that portions of normal bone are replaced either by weaker bones or fibrous tissue. Other X-ray findings may include bowing of the bone, thinning of certain structures or expansion of other bony structures. Sometimes, other imaging tests, such as a computed tomography (CT) scan or magnetic resonance imaging (MRI), may be needed. The treating physician may request a biopsy (a small tissue sample) of the affected site. As this is a rare condition, a diagnosis of fibrous dysplasia would include ruling out other conditions such as a nonossifying fibroma, a unicameral bone cyst and an aneurysmal cyst.
What are the treatment options for fibrous dysplasia?
While there is currently no known cure for fibrous dysplasia, there are palliative therapies to assist in the management of fractures and prevention of deformities. Specialized techniques are often required in order to restore optimal alignment and bony integrity. Generally, an implant that protects the entire affected area is required to minimize delayed complications. Fixator-assisted nailing and fixator-assisted plating are two surgical techniques often used to address the bone deformities and limb length discrepancies that can arise with fibrous dysplasia.
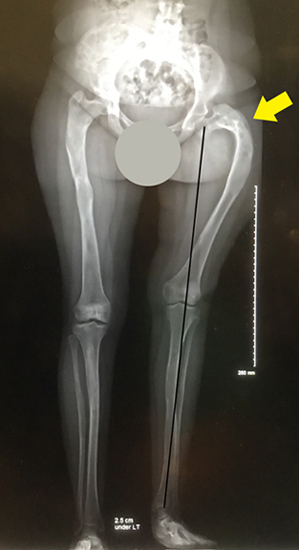 This X-ray shows how the hip & femur bone were deformed as a result of fibrous dysplasia.
This X-ray shows how the hip & femur bone were deformed as a result of fibrous dysplasia.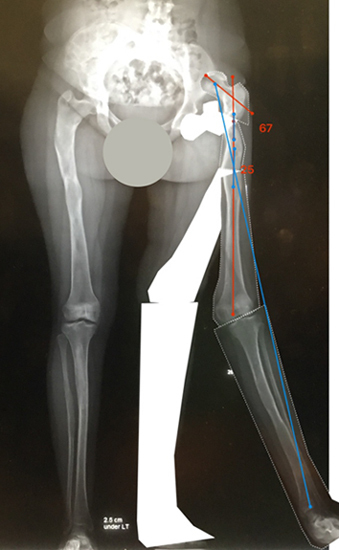 Using the International Center for Limb Lengthening’s
Using the International Center for Limb Lengthening’s 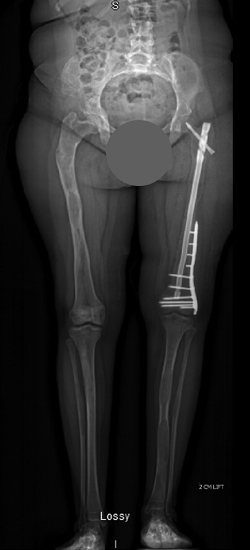 Through a combination of fixator assisted nailing and plating techniques, the surgery to correct the bone deformity was performed in two stages, without the need for any
Through a combination of fixator assisted nailing and plating techniques, the surgery to correct the bone deformity was performed in two stages, without the need for any If there is a fracture of the long bones of the legs, a rod is usually used in repair. Larger lytic lesions may require the use of bone graft. The source of the bone graft may be the patient themselves (autogenous graft) or from a donor (allograft), depending on the size of the lesion.
There is currently no medication to reverse or delay the progression of fibrous dysplasia. Some medications may be appropriate for management of specific symptoms. For example, intravenous bisphosphonates (a class of medicines that inhibit the cells responsible for breaking down bone) may assist in treating associated bone pain. Repeated visits may be needed, because fibrous dysplasia can recur. An endocrinologist will assist in the management of any associated symptoms, such as precocious puberty in girls, thyroid or pituitary conditions, etc.
Why choose the International Center for Limb Lengthening for the treatment of fibrous dysplasia?
The International Center for Limb Lengthening helps address orthopedic issues that arise from fibrous dysplasia. Limb lengthening and deformity correction are complex processes. Your doctor at the International Center for Limb Lengthening will take the time to make sure you understand all of your options and then will customize your treatment to meet your specific needs. Our patients benefit from our team-centered approach with world-renowned surgeons and specialized physician assistants, nurses and physical therapists. We help patients with fibrous dysplasia achieve their best possible orthopedic result.